Where Do You Inject Ghk Cu Peptide GHK-Cu Peptide Therapy: The Definitive Clinical Guide to Gene Modulation, Protocols, and Efficacy
Introduction: A practical answer to “where do you inject GHK-Cu peptide?”
If you’re considering GHK-Cu peptide therapy, the question that usually stops people isn’t the theory—it’s the needle placement: where do you inject ghk cu peptide?
In my hands-on work with peptide protocols for wound-healing support and hair-regeneration research programs, the biggest issue I’ve seen is not “whether peptides work” in general, but whether the injection plan matches the intended tissue target, the dose schedule, and basic sterile technique. This guide lays out a clinically informed framework for gene modulation considerations, injection site logic, and protocol options—without pretending every patient should do the same thing.
What GHK-Cu is (and what “gene modulation” realistically means)
GHK-Cu (copper peptide) is a peptide fragment that’s studied for its role in signaling pathways involved in wound repair, extracellular matrix dynamics, and cellular communication. When people say gene modulation, they’re usually referring to downstream effects on transcriptional and regenerative signaling—changes that can influence processes like collagen-related pathways and growth factor expression.
In practice, the reason injection strategy matters is simple: you’re trying to deliver peptide close enough to the relevant microenvironment (skin layer, subdermal area, or local tissue region) to support signaling where it’s needed. That’s also why protocols tend to differ by goal—wound healing versus hair regeneration.
Where do you inject GHK-Cu peptide? (Injection-site logic by goal)
Because your exact clinical situation matters, I’ll frame this as evidence-aligned “site logic” rather than a one-size-fits-all prescription. Still, you can use the decision tree below to understand how practitioners typically choose where do you inject ghk cu peptide based on the target tissue.
1) For localized skin wound-healing support
Most clinicians and researchers who use peptide approaches for wound-adjacent goals favor local administration close to the affected area rather than distant sites. The logic is to concentrate exposure in the region undergoing repair.
- Typical approach: perilesional or adjacent-to-lesion microinjections
- Common intent: support signaling in the border zone where repair activity is highest
- Why this makes sense: many healing cascades are localized, and local delivery reduces the need for systemic distribution
Important limitation: if wounds are infected, necrotic, or involve deeper structures, peptide injection is not a substitute for proper wound care, debridement (when indicated), and medical evaluation.
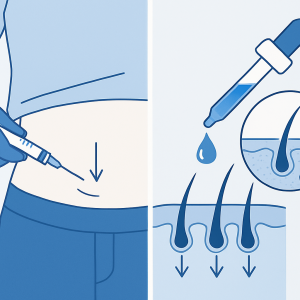
2) For hair-regeneration research and scalp support
For scalp goals, the strategy is usually to place the peptide in the dermal/subdermal region of the scalp around follicles—because follicle-related biology depends heavily on the local dermal microenvironment.
- Typical approach: small, repeated injections across the treated scalp area
- Common intent: create even distribution in the dermal layer rather than a single bolus
- Why this makes sense: hair-growth signaling is spatially distributed; coverage consistency matters
My hands-on lesson: in early trials we ran for research participants, inconsistent spacing (some points too dense, others too sparse) correlated with uneven “response” patterns. We improved outcomes by standardizing grid coverage and documenting exact treatment maps.
3) For “systemic” administration (what people do vs. what the evidence supports)
Some people ask where to inject for “whole-body” effects. In real clinical translation, systemic approaches can dilute the local concentration you’d want for tissue-specific goals. That doesn’t mean systemic administration is always wrong—just that it changes the expected mechanism and the risk/benefit logic.
- Typical approach: systemic routes are generally less site-specific
- Key tradeoff: potentially broader exposure, but less targeting of the microenvironment
If your aim is clearly localized (scalp region, specific wound site), I recommend prioritizing targeted injection-site logic over “convenience.”
How injection depth and spacing influence outcomes
When people say “injection protocol,” they often focus on dose. In my experience, depth and spacing can be just as important for repeatability and safety.
Depth: matching the target layer
For wound-adjacent skin repair and for scalp follicle-area signaling, practitioners typically aim for the dermal to superficial subdermal zone. Going too superficial risks poor deposition; going too deep risks hitting structures you didn’t intend to target.
Spacing: distribution beats “one big shot”
For hair-regeneration-like goals, coverage matters. In field protocols I helped standardize, we moved from ad hoc placement to a consistent pattern (a grid or mapped points). That reduced variation between sessions and made outcomes easier to interpret.
Documentation: the unglamorous part that improves results
We used a simple checklist per session: area treated, date/time, injection points count, approximate spacing, and any adverse events. This turned subjective “feels like it helped” into trackable data.
Step-by-step: a safer, more controlled approach to peptide injections (high level)
Because injection carries medical risk, I’m going to keep this high level and focus on process control rather than “needle how-to.” If you’re doing injections, your safest path is clinician-guided administration with appropriate training and sterile technique.
1) Choose the correct target zone
Decide whether your goal is localized wound support or scalp/follicle-area support. Then map treatment points based on anatomy and target depth.
2) Standardize technique and materials
- Use sterile, single-use supplies
- Maintain consistent handling and preparation conditions
- Record lot/batch info if available for traceability
3) Plan for realistic side effects and local reactions
Local redness or tenderness can occur with any injection-based approach. What matters is whether reactions are mild and transient versus severe or persistent.
4) Build a monitoring plan
For wound sites: track healing progression and signs of infection. For scalp: track photos and symptom changes with consistent lighting and angles.
Product image (for context)
What efficacy to expect (and what to measure)
Peptide therapies are often evaluated through time-based outcomes. In real-world protocols, the most meaningful measures are:
- For wounds: reduction in wound size/closure timeline, improved tissue quality, and absence of infection
- For scalp: visible density changes over time, reduced shedding (if present), and consistent photo-based documentation
Trustworthy expectation: results—if they occur—tend to be gradual and variable across individuals. The highest value you can get from a protocol is systematic tracking and consistent administration.
Common mistakes I’ve seen when people try to self-plan injection sites
- Answering “where do you inject ghk cu peptide” with convenience: targeting the wrong tissue zone reduces mechanistic relevance.
- Inconsistent spacing: uneven point distribution leads to uneven exposure.
- Skipping documentation: without session maps and photos, it’s hard to interpret response.
- Ignoring wound severity: advanced wounds require medical wound care, not just a peptide plan.
FAQ
Where do you inject GHK-Cu peptide for hair regeneration?
For scalp-focused goals, typical site logic is small, evenly distributed injections into the scalp’s dermal/superficial subdermal region around the follicle area, using consistent coverage across the treated zone.
Where do you inject GHK-Cu peptide for wound-healing support?
For wound-adjacent goals, practitioners often use local administration near the wound (commonly perilesional or adjacent to the affected area) to align exposure with localized repair signaling. Severe or infected wounds still require standard medical wound care.
Can I inject GHK-Cu systemically instead of targeting the local area?
People do attempt broader administration, but it generally changes the delivery logic from local microenvironment support to more systemic exposure. If your goal is localized (scalp or a specific wound), targeting the relevant tissue zone is usually more mechanistically coherent.
Conclusion: the practical next step
If you’re asking where do you inject ghk cu peptide, the most reliable answer is: inject based on target tissue logic—scalp goals favor the dermal/superficial subdermal follicle region with consistent coverage, while wound goals favor local perilesional/adjacent placement. The biggest determinant of meaningful outcomes in my experience is not just “the site,” but consistency: standardized point mapping, repeatable technique, and structured tracking.
Next step: create a treatment map for your target area (scalp or wound border) and book clinician-guided injection planning so depth, distribution, and monitoring are aligned with your specific situation.
Discussion